2026: Volume 7, Issue 1
Current Issue
 Abstract
Abstract  PDF
PDFIsolated Interrupted Inferior Vena Cava (IVC) With a Structurally Normal Heart
Vikranth Bapu Anna Venugopalan1, Shaswati Dey2
1Consultant Neonatologist with expertise in Paediatric Cardiology, Neonatal Unit, Midland Metropolitan University Hospital, Sandwell & West Birmingham Hospitals NHS Trust, Birmingham, UK
2Paediatric Trainee, Neonatal Unit, Midland Metropolitan University Hospital, Sandwell & West Birmingham Hospitals NHS Trust, Birmingham, UK
*Corresponding author: Vikranth Bapu Anna Venugopalan, Consultant Neonatologist with expertise in Paediatric Cardiology, Birmingham City Hospital, Sandwell & West Birmingham Hospitals NHS Trust, Birmingham, UK, E-mail: [email protected]
Received Date: December 15, 2025 Publication Date: February 20, 2026
Citation: Vikranth Bapu AV, Dey S. (2026). Isolated Interrupted Inferior Vena Cava (IVC) With a Structurally Normal Heart. Neonatal. 7(1):29.
Copyright: Vikranth Bapu and Dey S. © (2026).
ABSTRACT
We present a term infant with an isolated haemodynamically insignificant interrupted IVC with a structurally normal heart which was diagnosed antenatally and confirmed postnatally. Antenatal scan showed evidence of an interrupted IVC with venous return via an Azygos vein draining into the Superior Vena cava (SVC) with a structurally normal heart with no evidence of left atrial isomerism. Interrupted IVC with azygos continuation typically has a benign prognosis due to compensatory venous flow. It is important to be aware of this condition if there is a need for central venous catheter placements for any other reason. The infant was discharged and reassured the family about a benign prognosis and no restrictions from a cardiology perspective.
ABSTRACT
We present a term infant with an isolated haemodynamically insignificant interrupted IVC with a structurally normal heart which was diagnosed antenatally and confirmed postnatally. Antenatal scan showed evidence of an interrupted IVC with venous return via an Azygos vein draining into the Superior Vena cava (SVC) with a structurally normal heart with no evidence of left atrial isomerism. Interrupted IVC with azygos continuation typically has a benign prognosis due to compensatory venous flow. It is important to be aware of this condition if there is a need for central venous catheter placements for any other reason. The infant was discharged and reassured the family about a benign prognosis and no restrictions from a cardiology perspective.
BACKGROUND
Interrupted inferior vena cava (IVC) is a rare congenital anomaly that may occur in isolation or with other congenital heart defect or systemic anomalies. Interrupted IVC is very rare and often associated with heterotaxy syndromes with bilateral left sidedness – a condition called Left Atrial Isomerism which is associated with Atrioventricular Septal Defects (AVSD), Partial Anomalous Pulmonary venous connection (PAPVC) and pulmonary stenosis. They are associated with polysplenia. Isolated interrupted IVC without associated defects is rare and generally asymptomatic due to the normal venous return via Azygos vein into SVC. We present a term infant with an isolated, hemodynamically insignificant interrupted IVC, diagnosed antenatally and confirmed postnatally.
CASE PRESENTATION
A term baby was born at 39+0 weeks via elective cesarean section for footling breech presentation with a birth weight of 3.4 kg, required no resuscitation and was asymptomatic with no respiratory distress. He was diagnosed to have a congenital venous anomaly, an isolated interrupted IVC on the routine antenatal screening.
Physical examination revealed no dysmorphic features aside from bilateral positional talipes. Initial pre- and post-ductal oxygen saturation readings were 95% and 100%, respectively, normalising to 99% and 98%. The infant was formula-fed, passed urine, and opened bowels within 24 hours. Mild jaundice was observed but required no treatment.
INVESTIGATIONS
Antenatal ultrasound identified an isolated interrupted IVC, prompting postnatal evaluation. Antenatal detection of this condition is paramount which prompts to detailed systematic postnatal evaluation to exclude heterotaxy syndromes such as left atrial isomerism which is associated with Atrioventricular Septal defects (AVSD), Partial Anomalous Pulmonary venous connection (PAPVC) and Pulmonary stenosis.
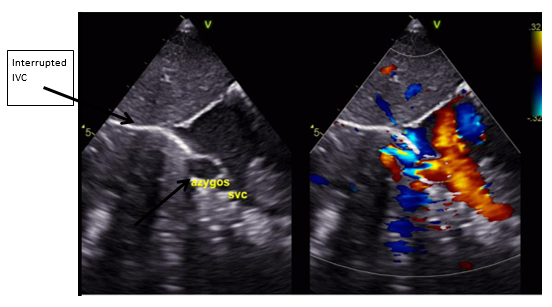
Postnatal ECHO revealed an Interrupted IVC (Figure 1) with venous return via the azygos vein (Figure 2 & Figure 3), draining into the superior vena cava (SVC), hepatic veins draining directly into the right atrium (RA), SVC draining into the RA and a small patent foramen ovale (PFO) with left-to-right shunting with normal cardiac anatomy with no abnormalities of the valves, aortic arch, outflow tracts, and no outflow tract obstruction.
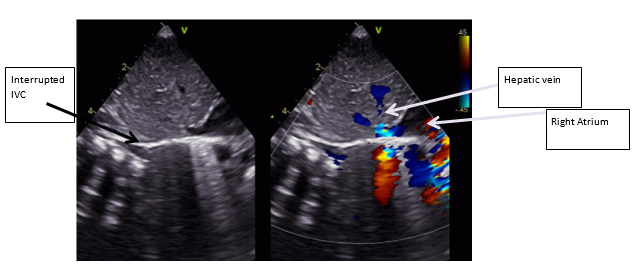
Figure 1: Subcostal echocardiographic view demonstrating absence of Retrohepatic IVC (Interrupted IVC) with hepatic venous drainage directly into the right atrium.
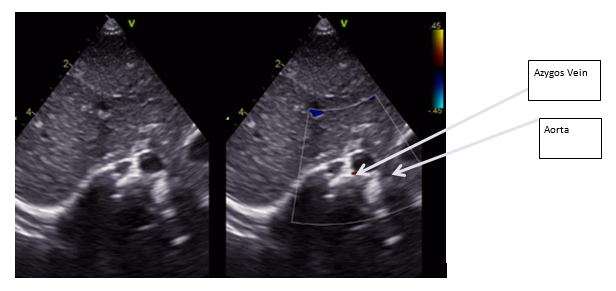
Figure 2: Subcostal echocariographic situs view showing Azygos vein instead of IVC (IVC is usually seen on the right side and more superiorly).
These findings confirmed a hemodynamically insignificant anomaly, with the azygos system compensating for the interrupted IVC without signs of venous congestion or systemic return compromise.
The infant was reviewed in the Pediatric Cardiology clinic subsequently and was asymptomatic from a cardiac standpoint. Repeat ECHO showed good biventricular systolic function, intact interatrial and interventricular septae, and absent IVC at the liver level (Interrupted IVC). Hepatic veins drained directly into the Right atrium (RA), while the azygos vein compensated with normal flow into the SVC. The pulmonary veins, numbering four, drained into the left atrium, and a single right-sided SVC drained into the RA. The aortic arch was unobstructed, and the pulmonary arteries were confluent and appropriately sized.
The absence of isomerism further supported the isolated nature of the interrupted IVC. To confirm hepatic drainage, a liver ultrasound was performed which confirmed the absence of the retro-hepatic segment of the IVC, three hepatic veins with normal directional triphasic flow, and no intra-abdominal abnormalities. It is important to be aware of this condition if there is a need for central venous catheter placements in the future for any other reason.
The infant was discharged from the Cardiology clinic and reassured the family regarding a benign prognosis and no restrictions from a cardiology perspective.
DISCUSSION
IVC formation during embryogenesis is complex, involving fusion and selective regression of the posterior cardinal, subcardinal, and supracardinal veins between the 6th and 8th gestational weeks [1]. Disruptions in this process lead to anatomical variants, such as interrupted IVC with azygos continuation, where the azygos vein compensates for the absent IVC segment [2,3].
In this case, the azygos system provided adequate compensation, allowing normal venous return to the heart without venous congestion or signs of right heart failure [3-9].
The pathogenesis of interrupted IVC is not fully understood, although failure of the subcardinal and supracardinal veins to fuse correctly during embryogenesis is implicated [1,6].
Interrupted IVC with azygos continuation typically has a benign prognosis due to compensatory venous flow. There are case reports of incidental finding of Isolated interrupted IVC with Pulmonary embolism [7-9].
Interrupted IVC is very rare and most often associated with heterotaxy syndromes with bilateral left sidedness – a condition called Left Atrial Isomerism or polysplenia syndrome. Isolated interrupted IVC with structurally normal heart is even rarer and only few cases have been reported in the literature. This was confirmed with postnatal detailed cardiac assessment including an echocardiogram and an abdominal ultrasound. Interrupted IVC has a benign course due to the normal venous return to the heart via Azygos vein. It is important to be aware of this condition if there is a need for central venous catheter placement in later life.
CONCLUSION
This case presents a term neonate with an isolated interrupted IVC identified antenatally and confirmed postnatally through echocardiography. The interruption, with compensatory azygos continuation, was hemodynamically insignificant, allowing the infant to remain asymptomatic. Postnatal imaging confirmed the absence of additional anomalies, and the prognosis remains positive. No restrictions were imposed, and the child is expected to lead a normal life. Long-term monitoring will ensure venous patency and prevent complications, although none are anticipated.
This case highlights the value of thorough antenatal and postnatal evaluation for identifying isolated interrupted IVC, enabling timely follow-up and supporting family education for ongoing well-being. It also highlights the importance of Antenatal detection and postnatal assessment to rule out associated cardiac and abdominal anomalies. Interrupted IVC is commonly associated with Isomerisms and this was ruled out in this case and highlighted the isolated Interrupted IVC with venous return via an Azygos vein draining into the SVC and thereby retaining a normal venous circulation.
Learning points/Take home messages
- Isolated interrupted IVC is rare
- Thorough evaluation to review the structure of the heart to rule out associated structural heart abnormalities such as Isomerism
- Interrupted IVC with azygos continuation typically has a benign prognosis due to compensatory venous flow
- Timely follow up and reassurance to the family with education is important for ongoing wellbeing of the child
PARENTAL CONSENT
Written Informed consent was obtained from the parents for publication of this case and accompanying images.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest related to this article.
REFERENCES
- Sadler TW. (2018). Langman's Medical Embryology. 14th ed. Philadelphia: Wolters Kluwer.
- Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH. (2000). Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 20(3):639–652.
- Perloff JK. Congenital anomalies of the inferior vena cava: Review. Am J Cardiol. 2011;108(8):1177-1183.
- Gayer G, Luboshitz J, Hertz M, Zissin R, Bass A, Rosenberger A, et al. (2003). Congenital anomalies of the inferior vena cava revealed on CT in patients with deep vein thrombosis. AJR. American Journal of Roentgenology. 180(3):729-732.
- Ruggeri M, Tosetto A, Castaman G, Rodeghiero F. (2001). Congenital absence of inferior vena cava: a rare risk factor for idiopathic deep-vein thrombosis. Lancet. 357(9254):441.
- Kocica MJ, Radovic MB. (2022). Developmental anomalies of systemic veins in the human embryo. Ann Biomed Sci.;94(5).
- Shahverdi E, Keshavarzi R, Mazandarani M, Schneider C, Lange M. (2024). Suprarenal interrupted inferior cava with azygos continuation in a patient with pulmonary embolism: a case report. European Heart Journal. Case Reports. 8(11):ytae583.
- Giang do TC, Rajeesh G, Vaidyanathan B. (2014). Prenatal diagnosis of isolated interrupted inferior vena cava with azygos continuation to superior vena cava. Annals of Pediatric Cardiology. 7(1):49-51.
- Chen SJ, Wu MH, Wang JK. (2022). Clinical implications of congenital interruption of inferior vena cava. Journal of the Formosan Medical Association = Taiwan yi zhi. 121(10):1938-1944.